Traumatic stress (1). History of the formation and development of the concept of mental trauma
Traumatic stress is a special form of the general stress reaction. When stress overloads a person’s psychological, physiological, and adaptive capabilities and destroys defenses, it becomes traumatic, that is, it causes psychological anxiety. However, not every event can cause traumatic stress. Psychological trauma is possible if:
The occurring event is realized, that is, the person knows what is happening to him and why his psychological state has worsened;
What a person has experienced disrupts his usual way of life.
Traumatic stress is a special kind of experience, the result of a special interaction between a person and the world around him. This is a normal reaction to abnormal circumstances.
According to modern views, stress becomes traumatic when the result of exposure to a stressor is a disorder in the mental sphere, similar to physical disorders. In this case, in accordance with existing concepts, the structure of the “self,” the cognitive model of the world, the affective sphere, the neurological mechanisms that control learning processes, the memory system, and emotional pathways of learning are disrupted. In such cases, traumatic events act as a stressor - extreme crisis situations that have strong negative consequences, life-threatening situations for oneself or loved ones. Such events significantly disrupt the individual's sense of security, causing experiences of traumatic stress, the psychological consequences of which are varied. The fact of experiencing traumatic stress for some people causes them to develop post-traumatic stress disorder in the future.
Post-traumatic stress disorder is a non-psychotic delayed reaction to traumatic stress (such as natural and man-made disasters, combat, etc.) that can cause mental disorders in almost any person.
Thus, PTSD has two significant features that distinguish it from ordinary stress.
The first is that psychological, physiological and socio-psychological disorders continue after the cessation of the stressor, when there is already a calm way of life around the psychotraumatized person.
The second feature is that PTSD can occur several months, even years, after experiencing psychotrauma, that is, when the stressful state that arose because of it has long ended.
Psychiatric stress researchers and the International Classification of Diseases, Tenth Revision (ICD-10) highlight a number of conditions for the occurrence of PTSD and its symptoms:
The person has experienced a life-threatening event;
Reaction in the form of fear, horror, helplessness;
Obsessive mention of an experienced event;
Dreams about an experienced event;
Actions or sensations that reenact an event;
Psychological stress when mentioning a traumatic event.
Avoiding conversations related to trauma;
Avoiding places and people associated with the injury;
Remembering aspects of trauma;
Decreased interest in meaningful activities;
Feeling of alienation from others;
Inability to feel love;
Difficulty falling asleep;
Overvigilance;
Increased reaction to fear;
Sustained mental stress.
Traumatic stress– a special form of general stress reaction. When stress overloads a person’s psychological, physiological, and adaptive capabilities and destroys defenses, it becomes traumatic, that is, it causes psychological anxiety. Not every event can cause traumatic stress. Psychological trauma is possible if:
– the event that occurred is conscious, that is, the person knows what happened to him and why his psychological state worsened;
– the experience destroys the usual way of life.
Traumatic stress is a special kind of experience, the result of a special interaction between a person and the world around him. This is a normal reaction to abnormal circumstances. Both children and adults who have experienced traumatic stress may sometimes appear abnormal or crazy when in fact they are not.
There are mechanisms of stress that are the same for children and adults. A certain degree of stress can even be beneficial, as it plays a mobilizing role and helps a person adapt to changing conditions. But if stress is strong and continues for too long, then it overloads a person’s adaptive capabilities and leads to psychological and physiological “breakdowns” in the body.
The most widespread concept is “psychological trauma”“received within the framework of the theory of post-traumatic disorder and crisis psychology that emerged in the late 80s. Psychological trauma is the experience of a special interaction between a person and the world around him. Psychological trauma - experience, shock. The most striking examples of psychological trauma are humiliation and threat to life and health.
Theoretical models of posttraumatic stress.
As a result of many years of research, several theoretical models have been developed, among which we can highlight: psychodynamic, cognitive, psychosocial and psychobiological approaches and the multifactorial theory of PTSD developed in recent years.
Psychological models include psychodynamic, cognitive and psychosocial models. They were developed during the analysis of the basic patterns of the process of adaptation of victims of traumatic events to normal life. Research has shown that there is a close connection between ways of getting out of a crisis situation, ways of overcoming post-traumatic stress (eliminating and avoiding any reminders of the trauma, being immersed in work, alcohol, drugs, the desire to join a mutual help group, etc.) and success subsequent adaptation.
According to the psychodynamic approach, trauma leads to disruption of the symbolization process. Freud viewed traumatic neurosis as a narcissistic conflict. He introduces the concept of a stimulus barrier. Due to intense or prolonged exposure, the barrier is destroyed, libidinal energy is shifted to the subject himself. Fixation on trauma is an attempt to control it. In the modern classical psychodynamic model, the following are considered as consequences of traumatization: regression to the oral stage of development, displacement of libido from the object to the Self, remobilization of sadomasochistic infantile impulses, the use of primitive defenses, automation of the Self, identification with the aggressor, regression to archaic forms of functioning of the “Super-I” , destructive changes in the I-ideal. It is believed that trauma is a trigger mechanism that actualizes childhood conflicts.
This model does not explain all the symptoms of a traumatic response, for example, constant acting out of the trauma. In addition, childhood trauma can be found in the experience of any person, which, however, does not predetermine the development of a maladaptive response to stress. In addition, classical psychoanalytic therapy is ineffective for treating this disorder.
Another aspect of individual characteristics of overcoming PTSD - cognitive assessment and reappraisal of traumatic experience - is reflected in cognitive psychotherapeutic models. The authors of this direction believe that the cognitive assessment of a traumatic situation, being the main factor in adaptation after trauma, will most contribute to overcoming its consequences if the cause of the trauma in the mind of its victim, suffering from PTSD, becomes external in nature and lies outside the personal characteristics of the person (broadly well-known principle: not “I’m bad”, but “I did a bad thing”).
In this case, according to researchers, faith in the reality of existence, in the existing rationality of the world, as well as in the possibility of maintaining one’s own control over the situation is maintained and increased. The main task in this case is to restore in consciousness the harmony of the existing world, the integrity of its cognitive model: justice, the value of one’s own personality, the kindness of others, since it is these assessments that are most distorted in victims of traumatic stress suffering from PTSD (Kalmykova, Padun, 2002).
Within the cognitive model, traumatic events are potential destroyers of basic ideas about the world and about oneself. A pathological reaction to stress is a maladaptive response to the devaluation of these basic ideas.
In the psychophysiological model, the response to trauma is the result of long-term physiological changes. Variability in responses to trauma is due to temperament.
According to modern data (Kolb, 1984; Van der Kolk, 1991, 1996), under stress, the turnover of norepinephrine increases, which leads to an increase in the level of plasma catecholamine, a decrease in the level of norepinephrine, dopamine, serotonin in the brain, an increase in the level of acetylcholine, the emergence of analgesic effect mediated by endogenous opioids. Decreased levels of norepinephrine and a drop in dopamine levels in the brain correlate with a state of mental numbness. This condition, according to many authors (Lifton, 1973; 1978; Horowitz, 1972; 1986; Green, Lindy, 1992), is central to the stress response syndrome. The analgesic effect mediated by endogenous opioids can lead to opioid dependence and seeking out traumatic-like situations. A decrease in serotonin inhibits the system that suppresses the continuation of behavior, which leads to a generalization of the conditioned response to stimuli associated with the original stressor. Suppression of the functioning of the hippocampus may cause amnesia for specific traumatic experiences.
The disadvantage of these models is that most studies have been conducted on animals or in vitro. They also do not take into account the dependence of the psychophysiological response on cognitive mediation, which was shown in the experiments of Lazarus.
The information model developed by Horowitz (1998) is an attempt to synthesize cognitive, psychoanalytic and psychophysiological models. Stress is a mass of internal and external information, most of which cannot be reconciled with cognitive schemes.
According to the psychosocial approach, the trauma response model is multifactorial, and the weight of each factor in the development of the stress response must be considered. It is based on Horowitz's model, but the authors and supporters of the model also emphasize the need to take into account environmental factors: factors of social support, stigma, demographic factors, cultural characteristics, additional stress. This model has the limitations of an information model, but the introduction of environmental factors allows for the identification of individual differences.
Until recently, the “two-factor theory” was the main theoretical concept explaining the mechanism of PTSD. It was based on the classical principle of conditioned reflex conditioning of PTSD (according to I.P. Pavlov) as the first factor. The main role in the formation of the syndrome is given to the traumatic event itself, which acts as an intense unconditional stimulus that causes an unconditional reflex stress reaction in a person. Therefore, according to this theory, other events or circumstances, neutral in themselves, but in some way associated with the traumatic event stimulus, can serve as conditioned reflex stimuli.
However, using the two-factor theory, it has been difficult to understand the nature of some symptoms unique to PTSD, such as “persistent return to experiences associated with the traumatic event.” These are symptoms of intrusive memories of the experience, dreams and nightmares about the trauma, and, finally, the flashback effect. In this case, it is almost impossible to establish which “conditioned” stimuli provoke the manifestation of these symptoms, so weak is their visible connection with the event that caused the trauma.
1.1. The concept of stress by G. Selye.1.2. The concepts of “trauma”, “traumatic stress”, “post-traumatic stress disorder”.
1.1. The concept of stress by G. Selye
The creation of the biological concept of stress was started by Hans Selye in 1936. He called balancing the body’s activity with constantly changing environmental conditions one of the main functions of the psyche. Thus, central to the concept of stress
G. Selye developed a homeostatic model of the body’s self-preservation and mobilization of resources to respond to a stressor. In this sense, stress is one of the natural human states. Stress (from the English stress - pressure, pressure) is any more or less pronounced tension in the body associated with its vital activity. We are talking about a set of stereotypical, phylogenetically programmed reactions of the body caused by exposure to various intense stimuli in our environment or difficult life situations. In their initial essence, the reactions of the body that arise are of an adaptive nature. And in this capacity, stress is an integral manifestation of life.
The starting points that cause stress are stressful events or stressors. Stressors are usually divided into physiological(pain, hunger, thirst, excessive exercise, high
and low temperature, etc.) and psychological(danger, threat, loss, deception, resentment, information overload, etc.). The latter, in turn, are divided into emotional and informational.
If we consider events as stressors, then they can be systematized by the amount of negative significance and by the time required for adaptation. Depending on this, critical life events, traumatic stress, everyday stressors or chronic stressors are distinguished (Pushkarev A.L. et al., 2000).
Based on the type of impact on a person, stress can be divided into the following types:
Systemic stress, reflecting the tension of predominantly biological systems. They are caused by poisoning, tissue inflammation, bruises, etc.
Mental stress that arises from any type of influence that causes an emotional reaction.
and processes in which, at least for a time, the relationship between the effort required and the resources available seems to be upset, and not in favor of the resources.
G. Selye identifies three main stages in the development of stress:
the first is the alarm stage, or the anxiety stage,
the second is the stage of resistance, or resistance,
the third is the stage of exhaustion.
by the third stage they return with triple strength.
If the stress factor is too strong or continues to act, then a stage of resistance begins, which is characterized by the almost complete disappearance of signs of anxiety; the level of body resistance is significantly higher than usual. At this stage, a balanced expenditure of adaptation resources is carried out. If the stress factor is extremely strong or acts for a long time, the stage of exhaustion develops.
At this time, the energy is exhausted, physiological and psychological defenses are broken. Signs of anxiety reappear.
According to G. Selye’s figurative comparison, these three phases of the general adaptation syndrome resemble the stages of human life: childhood (with the inherent low resistance and excessive reactions to stimuli at this age), maturity (when adaptation occurs to the most frequent influences and resistance increases) and old age (with irreversible loss of resistance and gradual decrepitude), ending in death.
Coping with stress includes psychological (this includes cognitive, emotional and behavioral strategies) and physiological mechanisms. If attempts to cope with the situation are ineffective, stress continues and can lead to pathological reactions. Under some circumstances, instead of mobilizing the body to overcome difficulties, stress can cause serious disorders (Isaev D.N., 2004).
1.2. The concepts of “trauma”, “traumatic stress”,
"post-traumatic stress disorder"
The scientific term “stress” has long been included in everyday language, they write about it in popular and fiction literature, and they are looking for ways to avoid and relieve this condition. However, it is necessary to distinguish between “normal” stress, which does not disrupt human adaptation, and traumatic stress. Traumatic stress occurs when the result of exposure to a stressor is
mental disorder.
In the early 80s. An independent research direction has emerged that deals with extreme overloads, their overcoming and consequences, as a result of which such concepts as “traumatic overloads”, “traumatic stress” or, simply, “psychological trauma” have emerged. But the concept of trauma, despite its frequent use, is defined mainly in general terms: an event of high intensity with a simultaneous lack of ability to adequately cope and exceeding the adaptive potential of the individual, which can result in adaptation disorders and stress-related disorders (Freedy J. R., Hobfoll S. E. , 1995). According to DSM-IV (Diagnostic and Statistical Manual of Mental Disorder - Psychiatric Classification Standard prepared by the American Psychiatric Association). A traumatic event occurs when it involves death, the threat of death, severe injury, or some other threat to physical integrity; Moreover, this event can affect a person directly or indirectly - through significant persons. But sometimes trauma also occurs due to the fact that a person witnesses the danger that threatens someone, the injury or death of a complete stranger. Such events fundamentally violate the individual’s sense of security, causing anxiety traumatic stress, the psychological consequences of which are varied.
Traumatic stress is a special kind of experience, the result of a special interaction between a person and the world around him. This is a normal reaction to difficult, traumatic circumstances, a condition that arises in a person who has experienced something that goes beyond ordinary human experience (Cherepanova E. M., 1997).
V. G. Romek, V. A. Kontorovich identify four characteristics of trauma that can cause traumatic stress:
1. The event that occurred is realized, that is, the person knows what happened to him and why his psychological state worsened.
2. This condition is caused by external reasons.
3. The experience destroys the usual way of life.
4. The event that occurred causes horror and a feeling of helplessness, powerlessness to do or undertake anything.
The psychological reaction to trauma includes three relatively independent phases, which allows it to be characterized as a process unfolding over time (Pushkarev A.L. et al., 2000).
First phase- phase of psychological shock - contains two main components:
1. Suppression of activity, disruption of orientation in the environment, disorganization of activities.
2. Denial of what happened (a kind of protective reaction of the psyche). Normally, this phase is quite short-lived.
Second phase- impact - characterized by pronounced emotional reactions to the event and its consequences. This can be intense fear, horror, anxiety, anger, crying, accusation - emotions characterized by immediacy of manifestation and extreme intensity. Gradually, these emotions are replaced by reactions of criticism or self-doubt. It proceeds along the lines of “what would have happened if...” and is accompanied by a painful awareness of the inevitability of what happened, recognition of one’s own powerlessness and self-flagellation. This phase is critical in the sense that after it either the “recovery process” begins, or fixation on the injury occurs and the subsequent transition of the post-stress state into a chronic form. In the latter case, the person remains in the second phase of response. With a successful emotional response, third phase- normal response phase. It can be presented in the form of a diagram (Fig. 1).
Rice. 1. Phases of recovery from a stressful state
Disorders that develop after experiencing psychological trauma affect all levels of human functioning (physiological, personal, level of interpersonal and social interaction), lead to lasting personal changes not only in people who have directly experienced stress, but also in their family members.
For some people, experiencing traumatic stress causes them to develop post-traumatic stress disorder (PTSD) in the future.
Post-traumatic stress disorder
(PTSD) is
a non-psychotic delayed reaction to traumatic stress that can cause mental disorders in almost any person. The range of phenomena that cause traumatic stress disorders is quite wide and covers many situations when there is a threat to one’s own life or the life of a loved one, a threat to physical health or the image of “I”.
Post-traumatic stress disorder (PTSD - Posttraumatic Stress Disorder) is defined as a complex of symptoms observed in those who have experienced traumatic stress. It is assumed that symptoms may appear immediately after exposure to a traumatic situation, or may occur many years later.
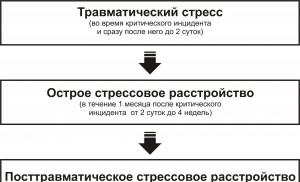
In accordance with the characteristics of the manifestation and course, three subtypes of post-traumatic stress disorders are distinguished (Romek V. G., Kontorovich V. A., 2004):
spicy, developing over a period of up to three months (it should not be confused with acute stress disorder, which develops
within one month after the critical incident);
chronic, lasting more than three months;
delayed, when the disorder occurred six months or more after the trauma.
Schematically the relationship between different stages of the formation of post-stress in terms of time of occurrence, duration and depth
violations by V. G. Romek, V. A. Kontorovich are presented as follows (Fig. 2).

Rice. 2. Stages of formation of post-stress disorders
The ravages of trauma continue to impact a person's entire life, disrupting the development of a person's sense of security and self-control. This causes strong, sometimes unbearable tension. And if this tension is not relieved, then the integrity of the psyche is in real danger. In general terms, this is the path along which the development of post-traumatic stress condition occurs.
Questions for self-control
Name the main types of stress.
What stages of stress development were identified by G. Selye?
What characteristics distinguish traumatic stress from “normal” stress?
What is the difference between traumatic stress and post-traumatic stress disorder?
Describe the phases of the psychological response to trauma.
What are the types of post-traumatic stress disorders depending on the characteristics of their course?
How are post-traumatic stress disorders different from post-traumatic personality disorders?
Formulate the stages of formation of post-stress disorders.
Exercise
Review the stress statements below. Determine which ones are false and which ones are true. Justify your point of view.
List of statements
Stress-related symptoms and psychosomatic illnesses cannot cause me real harm because they all exist only in my imagination.
Only weak people suffer from stress.
I am not responsible for the stress in my life. Stress is inevitable these days - we are all victims of it.
I always know when I'm overly stressed.
Sources of excessive stress are easy to recognize.
All people react to stress in the same way.
When I start to feel overly stressed, all I have to do is sit down and relax.
Isaev, D. N. Child medical psychology. Psychological pediatrics / D. N. Isaev. - St. Petersburg. : Speech, 2004. - 384 p.
Malkina-Pykh, I. G. Extreme situations: a reference book for a practical psychologist / I. G. Malkina-Pykh. - M.: Eksmo, 2005. - 960 p.
Romek, V. G. Psychological assistance in crisis situations / V. G. Romek, V. A. Kontorovich, E. I. Krukovich. - St. Petersburg. : Speech, 2004. - 256 p.
Selye, G. Essays on the adaptation syndrome / G. Selye. - M.: MEDGIZ, 1991. - 54 p.
Selye, G. Stress without distress / G. Selye. - M.: Progress, 1979. - 48 p.
The range of phenomena that cause traumatic stress disorders is quite wide and covers many situations when there is a threat to one’s own life or the life of a loved one, a threat to physical health or self-image. Disorders that develop after experiencing psychological trauma affect all levels of human functioning (physiological, personal, level of interpersonal and social interaction), lead to lasting personal changes not only in people who directly experienced stress, but also in eyewitnesses and members of their families. Post-traumatic stress disorders contribute to the formation of specific family relationships, special life scenarios and can affect the rest of life.
Traumatic stress- a special form of general stress reaction. When stress overloads a person’s psychological, physiological, and adaptive capabilities, it becomes traumatic, i.e. causes psychological anxiety. Traumatic stress is a special kind of experience, the result of a special interaction between a person and the world around him, it is a normal reaction to abnormal circumstances.
The term “post-traumatic stress syndrome,” which denoted a type of mental disorder caused by severe stress, was first introduced in 1980 by M. Horowitz et al. and included in the American diagnostic taxonomy OSM-III-P.
Emphasizing some features of long-term post-stress disorders, E. Linderman in 1944 proposed using the concept of “pathological grief” to define them. According to the author, this may include the subject’s abnormal reaction to misfortune, as a result of which various mental and psychosomatic disorders develop. “Pathological grief” is a syndrome that has specific psychopathological and somatic symptoms. It can develop immediately after a misfortune or after some time, it can be exaggeratedly expressed or barely noticeable. With appropriate treatment, according to the author, this pathological syndrome can successfully transform into a “normal reaction to grief” and then disappear altogether.
All disorders observed in victims of accidents are grouped by the author as follows:
- Psychogenically caused somatic disorders (a feeling of constriction in the throat, shortness of breath, muscle weakness, etc.).
- Preoccupation with the constant representation of loss.
- Feeling of longing.
- Reaction of hostility and irritability.
- Loss of previously inherent behavioral stereotypes.
Particular attention of clinicians in the second half of the 70s was attracted by the influence of wartime stress. Among the most common disorders of the long-term period in these cases were noted: repeated intrusive memories, which often took the form of vivid figurative ideas and were accompanied by oppression, fear, somatic disorders, a state of alienation and indifference with loss of normal interests and feelings of guilt; frightening dreams associated with previous military experiences; increased excitability and irritability. The abbreviation PTSD (Post traumatic stress disorder) is widely used in the literature to refer to post-traumatic stress disorder syndrome.
The basis of PTSD, according to most researchers on this issue, is mental trauma, designated as an “event” that can cause severe mental stress. In all cases, such an event is unusual for the individual and is accompanied by fear, horror, and a feeling of helplessness. A number of factors intensify mental trauma. The most significant of them are the immediate probability of death, identification with the victim, loss of social connections, and uncertainty of long-term consequences.
It is difficult to determine the pathogenetic mechanisms of PTSD. Currently, there are different views on them and, accordingly, several new approaches to their study. In this regard, E. Breg proposes to distinguish between psychological, biological, and complex models of pathogenesis. Among psychological models, the most interesting are the models proposed by M. Horowitz. He relied on the ideas of 3. Freud. Freud, examining soldiers who took part in the First World War who suffered from nightmares, suggested that these dreams reflect the primary localization of traumatic images, and their repetition is an infantile form of defense, when constant recollection of misfortune leads to the formation of a protective experience. Freud classified the disorders present in patients as neurotic (“traumatic neurosis”). He later suggested that in traumatic neurosis there are negative and positive reactions. The former seem to repress the trauma with suppression, avoidance and phobias, while the latter, on the contrary, remind of it in the form of memories, images, fixation.
In M. Horowitz, these groups of reactions correspond to a group of symptoms of denial and re-experiencing. The author defined the external influence factor as a “traumatic stress event” that carries completely new information that the individual must integrate into previous life experience. A clinical study found that denial is symptomatically manifested by amnesia, impaired attention, general mental retardation, and a desire to avoid any mention of trauma or associations associated with it. Symptoms of “re-experiencing” are characterized by recurring obsessive thoughts, sleep disturbances, and feelings of anxiety. Currently, the most promising theoretical developments of pathogenesis are those that take into account both psychological and biological aspects of the development of PTSD. In particular, L. Kold, summarizing the data of psychophysiological and biochemical studies in veterans of the Vietnam War, points out that as a result of extreme intensity and duration of stimulating influence, changes occur in the neurons of the cerebral cortex, primarily affecting the areas of the brain, associated with the control of aggression and the sleep cycle.
B. Kolodzin in one of his works means by post-traumatic stress, first of all, that a person has experienced a traumatic event. The other side of post-traumatic stress, in his opinion, relates to the inner world of the individual and is associated with a person’s reaction to the events he has experienced. Thus, when talking about PTSD, the author means that the person has experienced one or more traumatic events that deeply affected his psyche. These events were so different from all previous experiences or caused such great suffering that the person responds to them with a violent negative reaction. The normal psyche in such a situation seeks to alleviate discomfort: a person who has experienced such a situation radically changes his attitude towards the world around him. The author identifies the following clinical symptoms observed in post-traumatic stress:
- Unmotivated vigilance.
- "Explosive" reaction.
- Dullness of emotions.
- Aggressiveness.
- Impaired memory and concentration.
- Depression.
- General anxiety.
- Attacks of rage.
- Abuse of narcotic and medicinal substances.
- Unbidden memories.
- Hallucinatory experiences.
- Insomnia.
- Thoughts about suicide.
- "Survivor's Guilt."
In its modern form, the diagnostic criteria for post-traumatic stress disorder are most fully represented by the DSM-III-R disease classification.
- Post-traumatic stress disorder occurs as a result of mental trauma, an “event” that goes beyond normal experience and is a severe stress for any person (a serious threat to the life or health of children, close relatives, friends).
- The mental trauma (“event”) that caused PTSD is re-experienced by the victim in at least one of the following forms:
- persistent or episodic depressing memories of mental trauma;
- frequent repeated depressing thoughts associated with the “event”;
- a sudden feeling that “the event and what preceded it are being repeated again (including sensations, illusions, hallucinations);
- significant psychological oppression if current events resemble or are symbolically associated with mental trauma, including objects, dates, etc.
- Constant avoidance of anything that may be associated with the “event” or remind of it, as well as general mental retardation (at least 3 points):
- avoid situations or actions that may trigger memories of psychological trauma;
- the desire to get away from thoughts and feelings associated with mental trauma;
- inability to reconstruct important details related to the injury;
- significant loss of interest in previously important aspects of activity (in children - loss of speech and self-care skills);
- feelings of alienation and indifference to others;
- a noticeable decrease in the level of positive affective experiences (inability to experience feelings of love, joy);
- uncertainty about the future (inability to make a career, get married, have children or live long).
- Symptoms of increased excitability that were absent before mental trauma (at least 2 points):
- difficulty falling or staying asleep;
- irritability or angry outbursts;
- difficulty concentrating;
- increased caution;
- increased fearfulness;
- physiological reactions when mentioning an “event” or accompanying circumstances.
- Duration of symptoms included in sections B.C.D. must be at least one month. In this case, we may be talking about the presence of post-traumatic stress disorders - PTSD syndrome. Seizures that develop no earlier than six months after the injury are usually classified as specifically delayed. Although these criteria have been successfully used in the diagnosis of PTSD, critical review and testing of their validity and reliability is ongoing. Let us move on to consider the problem of post-traumatic stress disorders in Russian psychology. In Russian literature, the problems of the psychological consequences of natural disasters, catastrophes and military operations are analyzed mainly from the perspective of the dynamics of psychopathological manifestations. The result of many years of work by scientists was the advancement of the concept of an individual barrier to mental adaptation. In recent works, mainly from the perspective of this concept, the psychological consequences of natural disasters and catastrophes are analyzed. Their classification includes:
- Non-pathological (physiological) reactions.
- Psychogenic pathological reactions.
- Psychogenic neurological conditions.
- Reactive psychoses.
According to many authors, psychogenic disorders can arise during extreme conditions and disappear on their own when a person’s adaptation to it is completed (especially non-pathological reactions, while others require medical assistance). In some cases, both non-pathological reactions and pathological ones tend to transform into more severe forms of mental disorders several months after extreme exposure. Yu.A. Aleksandrovsky and other authors identify the following main clinical manifestations of different stages of psychogenic and mental disorders.
- For non-pathological neurotic manifestations: asthenic disorders, anxious tension, autonomic dysfunction, night sleep disorders, the emergence and decompensation of psychosomatic disorders, lowering the threshold of tolerance to harm. These phenomena are characterized by partiality, the symptoms are not combined into syndromes, there is the possibility of their complete self-correction.
- For neurotic reactions: controlled feelings of anxiety and fear, neurotic disorders, decompensation of personality-typological characteristics.
- For neuroses: stabilized and clinically developed neurotic states, a predominance of depressive, neurasthenic disorders, severe psychosomatic (neurosis-like) disorders.
- With pathological personality development: stabilization and development of personality changes, loss of connection between neurotic disorders and the causes that cause them.
Traumatic stress is a special form of the general stress reaction. When stress overloads a person’s psychological, physical, and adaptive capabilities and destroys defenses, it becomes traumatic, i.e. causes psychological anxiety. Psychological trauma is possible if: - the event that occurred is conscious, i.e. the person knows what happened to him and why his psychological state worsened; - the experience destroys the usual way of life.
Traumatic stress is a special kind of experience, the result of a special interaction between a person and the world around him. This is a normal reaction to abnormal circumstances.
1. The traumatic event is persistently experienced again and again. This can occur in various forms: - Repetitive and violently erupting memories of the event, including images, thoughts or ideas. Recurring nightmares about the event
Actions or feelings consistent with those experienced during the trauma. These include illusions, hallucinations and so-called flashback memories.
Intense negative feelings when confronted with something resembling (symbolizing) the traumatic event
Physiological reactivity if something resembles or symbolizes a traumatic event: stomach cramps, headaches. and etc.
2. Stubbornly avoids everything that may be associated with the trauma: thoughts or conversations, actions, places or people that remind you of the trauma.
3. There is an inability to remember important episodes of trauma, i.e. a person cannot remember some episodes of what happened to him.
4. There is a marked decrease in interest in what previously occupied him, the person becomes indifferent to everything, nothing captivates him.
5. There is a feeling of detachment and alienation from others, a feeling of loneliness.
6. Dullness of emotions - inability to overcome strong feelings (love, hate)
7. There is a feeling of a shortened future, i.e. short life prospect, when a person plans his life for a very short time. The child cannot imagine that he will have a long life, family, career, children, etc.
Persistent symptoms of the following group appear: Sleep problems (insomnia or interrupted sleep, Irritability or angry outbursts, Memory and concentration problems, Hypervigilance, Exaggerated reactivity
Theories explaining the occurrence of traumatic stress.
American psychologist J. Yalom will consider all the psychological problems of stress from the point of view of death, freedom, isolation, meaninglessness. In a trauma situation, these themes do not appear abstractly, not as metaphors, but are absolutely real objects of experience. Thus, death appears to a person in two ways. A person witnesses the death of other people (acquaintances, strangers, relatives, loved ones) and finds himself faced with his own possible death.
In ordinary life, a person has psychological defenses that allow him to exist side by side with the thought that one fine moment nothing will matter to him. These psychological defenses are not created immediately. For the first time, the fear of death arises in a three-year-old child: he begins to be afraid to fall asleep, asks his parents a lot if they are going to die, etc. Subsequently, the child creates psychological defenses that appear in the form of basic illusions. There are three of them: the illusion of one’s own immortality, the illusion of justice and the illusion of the simplicity of the world’s structure. The destruction of basic illusions is a painful moment for anyone. And it is very important what comes after this. If a person can leave the world of although comfortable, but still illusions, into a dangerous, but still real world, it means that he has matured and has greatly advanced as a person. If he was unable to overcome this barrier, then, as a rule, he either concludes that the world is terrible, or builds other illusions that help him recreate and strengthen the belief of his own immortality. Religion often plays such a role.
G. Selye identifies three main stages in the development of stress.
The first stage is the alarm stage, or the stage of alarm, when the body's adaptive resources are mobilized. At this stage, the person is in a state of tension and alertness. This is preparation for the next stage, which is why sometimes the first stage is called “pre-launch readiness”. Physically and psychologically the person feels very good and is in high spirits. During this phase, diseases that belong to the category of so-called “psychosomatic” often pass: gastritis, colitis, stomach ulcers, migraines, allergies, etc. If the stress factor is too strong or continues to act, the next phase begins - the stage of resistance, or resistance. At this stage, a balanced expenditure of adaptation capabilities is carried out. A person develops optimal energy by adapting to changing circumstances. He feels quite tolerable, although without the elation characteristic of the first phase. If the stressor continues to act even longer, the third stage begins - the stage of exhaustion. At the stage of exhaustion, energy is exhausted, physiological and psychological defenses are broken. A person no longer has the opportunity to defend himself.
Post-traumatic reactions: cognitive, emotional, behavioral, somatic.
Cognitive reactions include recurrent dreams or nightmares about the disaster; replaying the events associated with the disaster in your mind so that it looks different; difficulty concentrating or remembering; revaluation of spiritual or religious views; persistent intrusive thoughts or memories about the disaster or loved ones who died in the disaster.
Emotional reactions include feeling numb, immersed, or isolated; a feeling of fear and anxiety when objects remind a person of the disaster, especially sounds and smells; a feeling that you have lost interest in everyday activities or that they do not bring you joy; feeling of constant depression; outbursts of anger or excessive irritability; a feeling of emptiness or hopelessness about the future.
Behavioral responses may include being overly concerned about one's own safety and the safety of one's family; isolation from other people; increased alertness and fearfulness; difficulty falling asleep or staying asleep; avoidance of activities reminiscent of the disaster, from visiting places or meeting people that evoke tragic memories; increased conflict with family members; staying constantly busy so as not to think about what happened; tearfulness or crying for no apparent reason.
Somatic reactions may include insomnia, headaches, stomach pain, muscle tension, rapid heartbeat and intermittent fever. As stress accumulates, symptoms may worsen, resulting in severe illness.