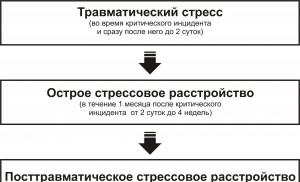
Instructions for use of the drug dexamethasone - composition, indications for use, side effects and analogues. Principles of treatment of cerebral edema
Dexamethasone in Israel is a fairly well-known and frequently used drug. It cannot be said that its use will help cure an existing disease. Rather, it will help the body cope with the problem on its own. Quite often used to raise white blood cells after chemotherapy.
Since it belongs to glucocorticosteroids, its main action is based on the binding of this hormone produced by the pituitary gland.
Indications for use
The spectrum of action of the drug is quite extensive. Accordingly, there are quite a lot of indications for its use. First of all, these are endocrine diseases, in particular insufficiency and hyperplasia of the adrenal cortex, thyroiditis.
It is also used in Israel for the treatment of diseases of the nervous system (postoperative period of treatment of brain tumors, strokes, inflammatory diseases of the meninges).
In ophthalmology it is prescribed for the treatment of conjunctivitis, keratitis, scleritis and other inflammatory processes, in the recovery period after eye injury and surgery.
Dexamethasone is also widely used during resuscitation in Israel. With its help, severe bronchospasm (with status asthmaticus), severe allergic reactions, including anaphylactic shock, are relieved.
The drug is also prescribed for blood diseases, including malignant ones: acute anemia, agranulocytosis, acute leukemia and leukemia.
The effectiveness of the drug for raising leukocytes after chemotherapy
The ability of this drug to influence the hematopoietic system makes it possible to use it to raise leukocytes after chemotherapy for cancer. Dexamethasone promotes the release of the most numerous group of white blood - neutrophils - into the blood. And the main task of these cells is to destroy bacteria in the blood and tissues. Also, the drug limits the migration of leukocytes to the affected area, thereby protecting them from destruction.
Contraindications
However, despite the wide spectrum of action of the drug, it also has a number of contraindications:
- Acute gastrointestinal diseases: ulcers, gastritis in the acute stage, colitis.
- Cardiovascular diseases - hypertension, heart failure. In patients who have suffered a myocardial infarction, the necrotic lesion may spread.
- Childhood. Since glucocorticosteroids affect the growth of a child, Dexamethasone is prescribed to children only for absolute indications and under constant medical supervision.
- Vaccination period. The drug cannot be used 2 months before vaccination and 3 weeks after it.
- Immunodeficiency diseases (HIV and AIDS).
- Pregnancy. Also, as in childhood, during pregnancy the drug is prescribed only for absolute indications.
Price and analogues
As for the cost, the drug is a fairly inexpensive medicine. The price for tablets varies between 100 - 200 rubles, and for ampoules 200 - 300 rubles (depending on the region).
Among the analogues of the drug, the most common are “Maxidex”, “Dexon” and “Farmadex”. These are medicines of a newer generation; their use is well tolerated and has minimal side effects. But you should remember that only the attending physician can prescribe a drug and select its analogues after a thorough examination of your body!
Side effects
Dexamethasone is usually quite easily tolerated. However, in some cases the following side effects may develop:
From the side of the heart:
- rhythm disturbance;
- rise in blood pressure;
- thrombosis.
From the gastrointestinal tract:
- loss of appetite (up to bulimia);
- flatulence;
- exacerbation of existing diseases of the gastrointestinal tract (pancreatitis).
From the endocrine system:
- increased blood glucose levels;
- moon-shaped face;
- suppression of the adrenal glands.
From the central nervous system:
- sleep disorders;
- attacks of dizziness;
- intense headache;
- in rare cases, patients experience seizures.
In addition to the above side effects, the medicine also affects the excretion of minerals from the body, in particular potassium and calcium. Therefore, when treating with this drug, it is necessary to regulate your diet taking into account the consumption of foods rich in these minerals. Conversely, sodium ions and water are retained in the body, and therefore diuretics are usually introduced into complex treatment.
Based on the foregoing, it can be noted that, being a broad-spectrum drug, “Dexamethasone” is used not only to treat a particular disease, but also to alleviate the condition and restore the body after a severe surgical intervention or other serious impact on the body, including including for raising leukocytes after chemotherapy.
Dosage form: injection Compound:For 1 ml:
active substance: dexamethasone sodium phosphate 4.37 mg(corresponding to 4.00 mg dexamethasone phosphate):
Excipients : glycerol 22.50 mg, disodium edetate dihydrate 0.10 mg, sodium hydrogen phosphate dihydrate 0.80 mg, water for injection q.s. up to 1.00 ml.
Description:Transparent, colorless or slightly yellowish liquid.
Pharmacotherapeutic group:Glucocorticosteroid ATX:H.02.A.B Glucocorticoids
S.01.B.A Corticosteroids
Pharmacodynamics:Dexamethasone is a synthetic hormone of the adrenal cortex with glucocorticosteroid action (GCS). It has anti-inflammatory and immunosuppressive effects, and also affects energy metabolism, glucose homeostasis and
(via negative feedback) on the secretion of hypothalamic activating factor and adrenocorticotropic hormone from the pituitary gland.GCS are fat-soluble substances and therefore easily penetrate into target cells through cell membranes. The binding of a hormone to a receptor causes conformational changes in the receptor and increases its affinity for DNA. The hormone-receptor complex enters the cell nucleus and binds to the regulatory region of the DNA molecule, also known as the glucocorticoid response element (GRE).
The activated receptor binds to GREs or specific genes and regulates messenger RNA (mRNA) transcription. The newly formed mRNA is transported to ribosomes, which then participate in the formation of new proteins. Depending on the type of target cells and cellular processes, the formation of new proteins can either be enhanced (for example, the synthesis of tyrosine transaminase in liver cells) or suppressed (for example, IL-2 synthesis in lymphocytes). Since receptors for GCS are found in all tissues, their action is realized in most cells of the body.
Effect on energy metabolism and glucose homeostasis: , along with insulin, glucagon and catecholamines, regulates the accumulation and expenditure of energy. In the liver, it stimulates the formation of glucose from pyruvate and amino acids and the formation of glycogen. IN peripheral tissues, particularly in muscles, reduces glucose consumption and mobilizes amino acids (from proteins), which are a substrate for gluconeogenesis in the liver. Direct effects on fat metabolism include central redistribution of adipose tissue and increased lipolysis in response to catecholamines.
Through receptors in the proximal tubules of the kidneys, it stimulates renal blood flow and glomerular filtration, suppresses the formation and secretion of vasopressin and improves the ability of the kidneys to excrete acids.
Increases the sensitivity of blood vessels to pressor agents.
In patients who have received long-term dexamethasone therapy and are exposed to stress after its discontinuation, dexamethasone use should be resumed due to the fact that induced adrenal insufficiency may persist for a period of time. several months after discontinuation of the drug.
Dexamethasone therapy may mask signs of infectious processes and signs of intestinal perforation.
Dexamethasone may aggravate the course of fungal infections, latent amoebiasis or pulmonary tuberculosis. Patients with acute pulmonary tuberculosis can be prescribed (together with anti-tuberculosis drugs) only in the case of a fulminant or severe disseminated process. Patients with inactive pulmonary tuberculosis receiving Dexamethasone therapy or patients with positive tuberculin tests should simultaneously receive therapy with anti-tuberculosis drugs.
Particular attention and careful medical supervision is necessary for patients with osteoporosis, hypertension, heart failure, tuberculosis, glaucoma, liver or kidney failure, diabetes mellitus, active peptic ulcers, fresh intestinal anastomoses, ulcerative colitis and epilepsy. Use with caution in the first weeks after acute myocardial infarction, as well as in patients with thromboembolism, myasthenia gravis, glaucoma, hypothyroidism, psychosis or psychoneurosis, as well as in elderly patients.
During dexamethasone therapy, decompensation of diabetes mellitus or transition from latent to clinically manifest diabetes mellitus is possible.
With long-term use, monitoring of serum potassium levels is necessary.
Vaccination with live vaccines is contraindicated during dexamethasone therapy.
Immunization with killed viral or bacterial vaccines does not give the expected increase in the titer of specific antibodies and therefore does not have the necessary protective effect. usually not used 8 weeks before vaccination and 2 weeks after vaccination.
Dexamethasone may increase susceptibility to or mask symptoms of infectious diseases. Chickenpox, measles and other infections can be more severe and even fatal in non-immunized individuals. Immunosuppression often develops with long-term use of GCS, but can also occur with short-term treatment.
Patients taking high doses of dexamethasone for a long time should avoid contact with infectious patients; If accidental contact occurs, prophylactic treatment with immunoglobulin is recommended.
Caution should be exercised when treating patients who have recently undergone surgery or bone fractures as it may delay the healing of wounds and fractures.
The effect of glucocorticosteroids is enhanced in patients with liver cirrhosis or hypothyroidism.
Intra-articular use of glucocorticosteroids may be accompanied by local and systemic effects.
Frequent use leads to destruction of articular cartilage and bone necrosis.
Before intra-articular injection, it is necessary to pump out and examine (for the presence of an infectious process) the synovial fluid from the joint. Injection of corticosteroids into the infected joint should be avoided. If septic inflammation develops in the joint after injection, appropriate antibiotic therapy is necessary. Patients should avoid putting stress on the joint into which the injection was made until the inflammatory process has completely resolved.
Glucocorticosteroids may alter the results of skin allergy tests.
Dexamethasone is used in children and adolescents only under strict indications. During treatment, strict monitoring of the growth and development of the child or adolescent is necessary.
Special information about some components of the drug
The drug contains less than 1 mmol (23 mg) sodium per dose.
Impact on the ability to drive vehicles. Wed and fur.:Dexamethasone does not affect the ability to drive vehicles or operate other technical devices that require increased concentration and speed of psychomotor reactions.
Release form/dosage:Solution for injection, 4 mg/ml.
Package:1 ml in dark glass ampoules (type
I). A colored dot is applied to the ampoule indicating the break line of the ampoule and a color coding ring.5 ampoules per blister made of PVC-aluminum foil.
5 blisters along with instructions for use are placed in a cardboard pack.
Storage conditions:At a temperature not higher than 25 °C.
Keep out of the reach of children.
Best before date:5 years.
Do not use the drug after the expiration date.
Conditions for dispensing from pharmacies: On prescription Registration number: P N012237/02 Registration date: 28.04.2011 / 14.05.2015 Expiration date: InstructionsContent
If a person has health problems, he immediately turns to pharmacological agents, so each of us must have a good understanding of what one or another of them is intended for. For example, Dexamethasone tablets have several areas of application, in addition, this medicine has many analogues. Read about the cases in which this drug can be prescribed, how it acts on the body and what substances it contains.
What is Dexamethasone
The drug belongs to the category of synthetic glucocorticoids. Available in tablets, eye drops, ampoules. The trade name and international nonproprietary name (INN) in the register of medicines (RMN) are the same - Dexamethazon. The medicine is intended to regulate carbohydrate, protein and mineral metabolism. The pharmacodynamics of tablets are characterized by the following actions:
- anti-inflammatory;
- antitoxic;
- desensitizing;
- immunosuppressive;
- antiallergic;
- anti-shock.
Compound
One flat round white tablet contains 0.5 mg of the main active ingredient - dexamethasone. They are packaged in 10 pieces in blisters or vials made of darkened glass. In addition, each Dexamethasone tablet contains the following auxiliary components:
- lactose monohydrate;
- colloidal anhydrous silica;
- corn starch;
- talc;
- povidone;
- magnesium stearate.
Indications for use
Dexamethasone can be prescribed for a huge number of diseases, divided into several groups. The tablets help against the following types of acute and chronic diseases of the musculoskeletal system:
- gouty and polyarthritic joint damage;
- epicondylitis;
- polyarthritis;
- rheumatism;
- synovitis;
- osteoarthritis;
- tenosynovitis;
- osteochondrosis;
- humeroscapular periarthritis;
- bursitis;
- ankylosing spondylitis;
- juvenile arthritis.

The hormone Dexamethasone can be prescribed for the following systemic connective lesions:
- rheumatoid arthritis;
- systemic lupus erythematosus;
- periarteritis;
- scleroderma;
- dermatomyositis.
If a person has a cold or allergies and has difficulty breathing due to increased mucus production, the doctor may also prescribe Dexamethasone or substitutes. Other tablets are prescribed for the following skin diseases:
- pemphigus;
- contact, toxic, seborrheic, bullous herpetiformis, exfoliative, atopic dermatitis;
- psoriasis;
- malignant weeping erythema.
Eye pathologies for which tablets are prescribed:
- allergic corneal ulcers;
- inflammation of the optic nerve;
- allergic conjunctivitis;
- indolent uveitis.
Tablets are prescribed for the following diseases of the hematopoietic system:
- erythrocyte, hypoplastic, erythroid, autoimmune hemolytic anemia;
- thrombocytopenic purpura;
- agranulocytosis;
- acute leukemia;
- lymphogranulomatosis.

Other diseases that can be treated with Dexamethasone tablets:
- congenital proliferation of the adrenal cortex;
- different types of cerebral edema;
- differential diagnosis of hyperfunction and tumor process of the adrenal cortex;
- elevated calcium levels;
- autoimmune kidney damage;
- prevention of implant rejection during transplantology;
- nephrotic syndrome;
- hepatitis;
- sarcoidosis;
- enteritis;
- fibrosis;
- Crohn's disease;
- acute alveolitis;
- ulcerative colitis;
- pulmonary forms of tuberculosis;
- multiple sclerosis;
- lung tumors;
- aspiration pneumonia.
Contraindications
According to the annotation, the tablets should not be used for:
- under 6 years of age;
- hypersensitivity to the components of the tablets;
- liver cirrhosis;
- stomach or duodenal ulcer;
- chronic hepatitis;
- osteoporosis;
- pregnancy, lactation;
- acute viral, fungal, bacterial infections;
- active form of tuberculosis;
- Cushing's syndrome;
- sore throat;
- esophagitis;
- acute psychosis;
- polio;
- some heart diseases;
- severe arterial hypertension;
- obesity 3-4 degrees;
- severe renal failure.

Side effects
As a result of taking Dexamethasone tablets, the following diseases and consequences may develop:
- acute pancreatitis;
- bronchospastic manifestations;
- nausea;
- liver damage;
- intestinal bleeding;
- abdominal pain;
- increased appetite;
- feces with blood;
- heartburn;
- esophagitis;
- vomit;
- thinning of the skin;
- allergy;
- acne;
- anaphylactic shock;
- sexual dysfunction;
- arrhythmia;
- increased sweating;
- adrenal insufficiency;
- the appearance of excess weight;
- Itsenko-Cushing syndrome;
- water retention;
- disruptions of the menstrual cycle;
- convulsions;
- bradycardia;
- visual and hearing disorders;
- increased intracranial pressure;
- psychosis;
- depression;
- dizziness;
- insomnia;
- irritability.
Dexamethasone - instructions for use
There are different schemes for using a hormonal drug based on what disease you want to overcome with its help. Your doctor should tell you how to take Dexamethasone tablets correctly, after making an accurate diagnosis. General recommendations:
- The initial dose of tablets for an adult per day is 0.5-9 mg.
- Maintenance intake – 0.5-3 mg per day.
- The maximum daily dose is 10-15 mg.
- If Dexamethasone tablets have a therapeutic effect, the dose is gradually reduced by 0.5 mg every three days to a maintenance minimum.
- The drug should be taken 2-4 times a day with meals.
- In case of an overdose of tablets, you should immediately consult a doctor.
- Be sure to check how Dexamethasone interacts with other medications prescribed to you, and whether taking it together will cause harm.

For oncology
As a rule, for some types of cancer, Dexamethasone can be prescribed to improve the patient’s general condition, as part of complex therapy. The tablets have relatively few side effects. Dexamethasone for oncology should be taken 7.5-10 mg per day. Taking pills is allowed only as prescribed by a doctor. It is preferable to be hospitalized at an oncology clinic during the admission period.
For bronchitis
Sometimes a drug is prescribed for this disease, but not in tablets. Dexamethasone for bronchitis and exacerbations of bronchial asthma is used in ampoules by inhalation. It helps prevent bronchospasm and relieve severe coughing attacks. 0.5 ml of medication is diluted in 2-3 ml of saline solution. Inhalation of the resulting product is given to adults and children three times a day for a week. This allows you to significantly alleviate the patient’s condition in a relatively short period of time.
For conjunctivitis
The drug is prescribed for many eye diseases, but not in tablets, but in drops. for conjunctivitis and other acute inflammations, treatment lasts two days. 1-2 drops are dropped into the eyes 4-5 times a day. If the disease is chronic, the course of treatment lasts from three to six weeks. In this case, 1-2 drops of Dexamethasone are instilled into the eyes twice a day. If the medicine gets on the cornea, a burning sensation is possible, which quickly passes, but this phenomenon is not considered a side effect.

For children
Depending on the diagnosis, 83-333 mcg of the drug per day is prescribed. The instructions for Dexamethasone recommend that treatment be carried out only according to strict indications and that the processes of development and growth of the child be strictly monitored throughout the entire period, because the pills at any time can provoke a slowdown and even a complete cessation. Therapy should be stopped gradually, reducing the dosage every three days to gradually eliminate hormones.
Dexamethasone analogs
Drugs with similar properties have a similar effect:
- Megadexane;
- Dexazone;
- Dekatron;
- Fortecortin;
- Dexaven;
- Pharmadex;
- Oftan Dexamethasone;
- Dexamed;
- Maxidex;
- Dexamethasonelong;
- Dexon;
- Medexol;
- Dexacort;
- Dexapos;
- Dexafar.

Price
You can purchase the drug only if you have a doctor's prescription. You can buy Dexamethasone at any pharmacy. In addition, the tablets are presented at affordable prices in the catalogs of specialized online stores that sell medicines. How much Dexamethasone costs depends on the form of release, the number of tablets, and the manufacturer. The price of a blister for 10 pieces in Moscow varies from 18 to 45 rubles.
Video
DEXAMETHASON
DEXAMETHASONUM H02A B02
KRKA
COMPOSITION AND FORM OF RELEASE:
Table 0.5 mg, No. 10 5.12 UAH.
Dexamethasone 0.5 mg
Other ingredients: lactose, corn starch, povidone, magnesium stearate, talc, colloidal anhydrous silica.
No. 3275 from 07/07/2003 to 07/07/2008
R-r d/in. 4 mg amp. 1 ml, No. 25 28.08 UAH.
Dexamethasone 4 mg
Other ingredients: disodium edetate, disodium phosphate dodecahydrate, water for injection, glycerol.
No. 3276 from 07/07/2003 to 07/07/2008
PHARMACOLOGICAL PROPERTIES: dexamethasone is a long-acting synthetic glucocorticosteroid that does not have mineralocorticoid effects. Has a powerful immunosuppressive and anti-inflammatory effect; exhibits antiallergic, antiexudative and antipruritic activity. Reduces vascular permeability, inhibits leukocyte migration, phagocytosis, kinin release, and antibody formation. It is approximately 25 times more active than hydrocortisone. The maximum effect with a single oral dose is achieved after 1-2 hours. Dexamethasone is well absorbed from the digestive tract, distributed in the tissues of the body. The volume of distribution is similar between groups. Metabolized in the liver. The maximum concentration of dexamethasone in the cerebrospinal fluid is determined 4 hours after intravenous administration and is 15-20% of the concentration in the blood plasma. Excreted by the kidneys, a small amount is excreted in bile. The half-life is 3-4.5 hours.
INDICATIONS: endocrine disorders - acute adrenal insufficiency; in preparation for surgery or in case of severe injury/illness in patients with adrenal insufficiency or insufficient adrenocortical reserve.
Shock when other treatments are ineffective, anaphylactic shock, shock in patients with adrenal insufficiency.
Brain edema due to primary brain tumors or brain metastases, craniotomy or traumatic brain injury.
Malignant diseases - palliative treatment of leukemia and lymphoma in adults, acute leukemia in children, hypercalcemia in patients with malignant tumors.
Diagnostic test to detect hyperfunction of the adrenal cortex.
Exacerbation of chronic obstructive bronchitis and asthma.
Intra-articular administration is used for severe forms of rheumatoid arthritis with impaired joint function and lack of effect from traditional therapy, and for other diseases accompanied by the development of synovitis with accumulation of effusion in the joint cavity (the drug is administered after aspiration of synovial fluid).
Local application (injection into the affected area) is indicated for sclerotic folliculitis, granuloma annulare and cutaneous sarcoidosis.
Subconjunctival, retrobulbar and parabulbar administration is indicated for threatened vision loss, allergic diseases, immunodeficiency, proliferative changes in the orbital fossa, sympathetic ophthalmitis and immunosuppressant therapy after corneal transplantation.
APPLICATION: oral administration
Parenteral use
Prescribed intramuscularly, intravenously or as an infusion in glucose solution or isotonic sodium chloride solution. The recommended initial dose for IV or IM administration is from 0.5 to 9 mg/day; if necessary, the dose is increased.
Local application
The recommended dose for intra-articular administration is from 0.4 to 4 mg once. Intra-articular injection can be repeated after 3-4 months; the same dose can be administered into the same joint no more than 3-4 times; Dexamethasone can be injected into no more than 2 joints at the same time. More frequent administration of dexamethasone may damage articular cartilage. The dose depends on the size of the affected joint. Typically, 2-4 mg of dexamethasone is injected into large joints, and 0.8-1 mg into small joints. 2 to 3 mg of dexamethasone is injected into the synovial bursa, 0.4 to 1 mg into the tendon sheath, and 1 to 2 mg into the tendons. For soft tissue infiltration, periarticular administration in a dose of 2 to 6 mg is recommended.
Children are prescribed IM. The dose for replacement therapy is 0.0233 mg/kg or 0.67 mg/m2, which is divided into 3 injections after 2 days on the third, or at a dose of 0.00776 to 0.01165 mg/kg or from 0.233 to 0.335 mg /m2 per day. When used for other indications, the recommended dose is 0.02776-0.16665 mg/kg or 0.833-5 mg/m2 every 12-24 hours.
CONTRAINDICATIONS: hypersensitivity to dexamethasone, osteoporosis, acute viral, bacterial or fungal infections (if appropriate therapy is not carried out simultaneously), Itsenko-Cushing syndrome. Relative contraindications are chronic renal failure, liver cirrhosis or chronic hepatitis, hyperthyroidism, psychosis or psychoneurosis, and old age. IM administration of dexamethasone is contraindicated in patients with idiopathic thrombocytopenic purpura.
SIDE EFFECTS: The risk of systemic and local side effects increases with prolonged use and increasing frequency of injections.
Local side effects include hyperemia, swelling, pain, and allergic reactions at the injection site. With prolonged use, stretching or rupture of the tendon, atrophy of the skin and subcutaneous fat at the injection site are possible.
Systemic side effects with rapid intravenous administration of dexamethasone in high doses may include facial skin flushing, irregular pulse, severe tachycardia, and stroke. Possible development of anaphylaxis. Rarely, generalized allergic skin reactions, sudden blindness, fever, paresthesia, mental disorders (impaired consciousness, agitation, anxiety, disorientation, euphoria, hallucinations, manic-depressive state, depression or paranoia) are observed. Glaucoma, cataracts, increased intraocular pressure and exophthalmos are possible.
SPECIAL INSTRUCTIONS: in case of adrenal cortex insufficiency in special situations (trauma, surgery), the dose of the drug is increased.
Dexamethasone is prescribed with caution to patients with ulcerative colitis, peptic ulcers of the stomach and duodenum, renal failure, systemic osteoporosis, myasthenia gravis. For infectious diseases, GCS should be prescribed in combination with antimicrobial drugs, for peptic ulcers - with antiulcer drugs. Caution is also necessary when prescribing dexamethasone to patients with severe hypertension, diabetes mellitus, mental illness, and glaucoma. With hypothyroidism, as well as with liver cirrhosis, the effect of the drug may be enhanced.
In children with long-term treatment, it is necessary to monitor the dynamics of growth and development.
During pregnancy (especially in the first trimester), the drug is prescribed only if the potential benefit to the expectant mother outweighs the possible risk to the fetus.
Due to the possible effect on growth and secretion of endogenous corticosteroids, it is recommended to discontinue breastfeeding during treatment with dexamethasone.
INTERACTIONS: Rifampicin, carbamazepine, phenobarbital, phenytoin, primidone, ephedrine or aminoglutethimide reduce the effectiveness of dexamethasone when used concomitantly. Dexamethasone reduces the therapeutic effect of antibacterial agents, antihypertensive drugs, coumarin anticoagulants, praziquantel and saluretics; increases the activity of heparin and albendazole.
Concomitant use of dexamethasone and β2-adrenergic receptor antagonists in high doses increases the risk of developing hypokalemia. In patients with hypokalemia, cardiac glycosides are more likely to cause arrhythmia, and their toxic effect increases. With simultaneous administration of oral contraceptives, the half-life of GCS may increase, which increases the likelihood of side effects.
The simultaneous administration of dexamethasone and ritodrine is contraindicated, as this may increase side effects.
The simultaneous administration of dexamethasone with metoclopramide, diphenhydramine, prochlorperazine, ondansetron and granisetron effectively prevents the development of nausea and vomiting during emetogenic chemotherapy with cisplatin, cyclophosphamide, methotrexate and fluorouracil.
OVERDOSE: in case of overdose (usually only a few weeks after it), Itsenko-Cushing syndrome may develop, as well as the side effects described above. There is no specific antidote. Symptomatic treatment is carried out. Hemodialysis is ineffective.
STORAGE CONDITIONS: in a dry place at temperatures up to 25 °C.
Circumstances change, principles never.
Multiple myeloma is an oncological disease that has several names. For example, if you see the term “generalized plasmacytoma” or “multiple myeloma,” you will know that they are the same disease. Just like Rustitsky-Kahlen disease. It belongs to the group of chronic leukemias.
The disease is a malignant tumor consisting of plasma cells (B-lymphocytes, elements responsible for the production of antibodies). A tumor develops through the proliferation (division) of B-lymphocytes.
The predominant site of localization of the oncological process is the bone marrow. Less often it has an extraosseous location. The disease is accompanied by bone marrow infiltration, bone tissue dissolution (osteolysis) and immunodeficiency.
Quite often, the first sign of the disease is bone pain and unexpected fractures. Then renal failure, hemorrhagic diathesis, polyneuropathy and amyloidosis develop. In the last stage, lymphoid tissue, intestines, and spleen may be affected.
Types of disease
According to international standards, there are several types of this pathology. The classification is based on clinical manifestations, biochemical blood tests and biopsy results. It is customary to highlight:
- Asymptomatic or smoldering myeloma.
- Symptomatic.
- MGUS (monoclonal gammopathy).
The most severe is symptomatic myeloma. Accompanied by renal failure, bone lesions, anemia, production of large amounts of monoclonal immunoglobulin and other symptoms.
When a B lymphocyte encounters an antigen, immunoglobulin is produced. When plasmacytoma develops, clonal B lymphocytes produce huge amounts of this globulin (called monoclonal globulin). It is this that is detected in a biochemical blood test.
The first and last types of myeloma do not have organic lesions characteristic of symptomatic myeloma. They are determined by the content of paraprotein in the blood plasma and punctate containing clonal plasmacytes (that is, B-lymphocytes formed by cell division).
Symptomatic myeloma progresses through 3 stages (I, II, IIIA, IIIB). The transition from one stage to another is justified by an increase in the mass of the tumor focus. The first stage describes the condition for any of these types of myeloma lesions. It is considered relatively mild, since there is no damage to bone tissue or internal organs, hemoglobin is slightly reduced, and the level of calcium in the blood is within normal limits. By the third stage, the bones begin to melt - this is a characteristic feature of the myeloma process.
Low hemoglobin levels, high calcium levels in the blood and kidney failure are all signs of the third stage of the process. Depending on the level of creatine in the blood, substages A and B are distinguished.
Myeloma is characterized not by bone destruction, but by lytic lesions (melting, resorption) of bone tissue.
Other classification

This disease is classified not only by severity and type of course, but also by several other criteria. So, myeloma is distinguished:
- Based on the composition of the cells involved in the tumor process, it is customary to distinguish between small cell, polymorphic, plasmablastic, and plasmacytic myeloma.
- Based on the ability to secrete paraproteins, they are distinguished: non-secreting tumors, diclon, Ben-Jones and G-, A-, M-myelomas. The last two types account for about 70% of all cases of plasmacytoma.
- According to the prevalence of the process.
Based on the degree of infiltration of bone marrow tissue, focal (nodular), diffuse-focal (diffuse-nodular) and diffuse (diffuse) myeloma are distinguished.
Rustetsky-Kahlen disease is characterized by a large number of lesions. But there are situations when degenerated plasma cells are concentrated in one place - this pathology is called solitary myeloma (plasmacytoma). In this case, monoclonal immunoglobulin is produced in extremely large quantities. And over time, such patients, even with treatment of the disease, develop symptoms of multiple myeloma.
Causes
Multiple myeloma, like most cancer pathologies (Ewing's sarcoma), does not have a clearly identified cause. This means that only a few factors have been identified that trigger or stimulate the tumor process.
The oncological process itself is considered low-malignant. That is, the disease takes a long time (20–30 years) from the moment of degeneration of the first progenitor cell to the appearance of clear symptoms.
Presumably the following factors lead to the development of the disease:
- Hereditary predisposition.
- Ionizing radiation.
- Environmental factors (chemical and physical carcinogens).
People get sick more often when they reach old age. Men are more susceptible to this disease than women. There are known cases of familial plasmacytoma.
The most common myeloma disease is believed to be caused by ionizing radiation and mutation of B lymphocytes. An indirect connection between this disease and work environment factors has been identified. As a result, it most often affects people associated with work in the oil refining industry, tanners, woodworkers and farmers.
Development

B-lymphocytes degenerate when they are mature, at the stage of their differentiation. Myeloma lesions are characterized by the presence of atypical plasma cells of varying degrees of maturity. Some have several nuclei and nucleoli, some are abnormally large. Pale colored plasma cells are found. But all are characterized by uncontrolled self-reproduction through division.
When such pathological tissue grows, it inhibits normal healthy hematopoietic tissue. This leads to a decrease in the blood's formed elements (erythrocytes, platelets and leukocytes). The level of certain chemicals that provide the body's immune response (for example, lysozyme, etc.) decreases.
Tumor cells are not able to provide a full protective function of the body, because normal antibodies are either not produced or are quickly destroyed.
The favorite localization of the myeloma tumor process is flat bones. These include:
- Scull.
- Pelvic bones and bone tissue of the ribs.
- Spinal tissues.
- Infiltrates containing tumor cells can also be found in other organs.
The x-ray image clearly shows the cavities formed in the areas where the tumor grows. Cavities are formed due to lysis (dissolution of cells) and resorption (reabsorption) of bone tissue. This type of resorption is called axillary.
The general clinical picture of the disease is caused by the proliferation of degenerated plasma cells and hypersecretion of monoclonal immunoglobulin.
Symptoms
The onset of the disease, the so-called preclinical period, proceeds without complaints, there are no subjective symptoms. The disease is detected randomly during a laboratory blood test.
As the disease progresses, symptoms associated with tumor damage to bones and internal organs appear. The most characteristic are:
- Bone symptoms.
- Nephropathy.
- Changes in the blood system (anemia, coagulation disorders, increased ESR).
- Immunodeficiency.
The first symptoms are, as a rule, complaints of pain in the spine, sternum, pelvic bones, ribs and clavicular area. Pain syndrome occurs first with palpation (pressure with fingers), then simply with movement.
Plasmocytosis of bone tissue, osteolysis and osteoporosis lead to the appearance of so-called spontaneous fractures, and those bones that normally break infrequently even with injuries and bruises. The first to be affected are the flat bones (ribs, clavicle fracture).
Fractures can also affect some parts of the spine. Most often, compression (non-displacement) fractures occur in the lumbar spine; the second most common fractures are the thoracic vertebrae.
Spinal fractures are fraught with serious consequences. Their symptoms depend on the damage done to the spinal cord. There may be shortening of growth and compression of the spinal cord. The latter leads to the appearance of symptoms of radiculopathy, impaired sensitivity, and the functioning of the pelvic organs (intestinal motility and bladder function) is inhibited. In addition to the spine and flat bones, joints are affected.
Amyloidosis is a disorder of protein metabolism that leads to the deposition of a specific complex, amyloid, in tissues. With amyloidosis of myeloma nature, patients complain of symptoms associated with damage to one or another organ (heart, kidneys, gastrointestinal tract, eyes). You may also develop:
- Heart or kidney failure.
- Dyspepsia.
- Mental disorders.
- Neuropathies.
- Sensory disturbances like stockings or gloves (although peripheral neuropathies are rare).
- Skin infiltrates appear.
- In rare cases, patients fall into a coma.
Disturbances in the blood system lead to hemorrhagic diathesis. These are capillary bleeding on the mucous membrane of the gums, nasopharynx, gastrointestinal tract, and uterus. Visually, bruises (hematomas) can be seen on the accessible mucous membranes. Anemia is characteristic of myeloma.
Due to paraprotein hypersecretion, ESR levels increase significantly (up to 80 mm/h) and blood viscosity increases. As a result, microcirculation in the most important organs of the human body is disrupted. These phenomena explain many neurological symptoms (including increased drowsiness, dizziness, headaches).
Generalized plasmacytoma leads to disturbances in the functioning of the organ of vision or to complete loss of vision. When the pathoprocess is localized in the bones of the skull, the cranial nerves, including the optic and oculomotor nerves, may also be affected. This leads to ophthalmoplegia (paralysis of the eye muscles).
Vision loss is associated with myeloma retinopathy (damage to the retina of the eyeball). In this case, thrombosis of the retinal venous network develops, and the optic nerve itself swells, up to its atrophy. The person gradually becomes blind.
The ability of the immune system to fight infectious agents (herpetic infections, coccal infections) decreases almost with the onset of the disease. It only intensifies with its development. Almost 50% of patients with multiple myeloma suffer from severe infectious complications. This condition, associated with increased sensitivity to bacterial infections, leads to the development of pyelonephritis, pneumonia and other inflammatory processes.
It is severe illnesses that often lead to the death of the patient, and not myeloma as such.
Diagnostics

The study for any disease begins with a general detailed blood test and a general urinalysis. A blood test can reveal changes in the content of formed elements. But the main indicator that can indicate further direction of research is the ESR level. A specific protein (serum paraprotein) is detected in the urine.
Diagnosis of multiple myeloma also includes:
- Blood tests (bio- and immunochemical).
- Biopsy analysis.
- Radiography.
- MRI, CT.
Biochemical analysis reveals increased concentrations in the blood of certain chemical compounds (creatinine, total protein, urea and some others). Immunochemistry determines the pathological paraprotein. X-rays reveal areas of bone tissue melting.
MRI allows one to differentiate generalized plasmacytoma from other bone lesions and identify lesions in other organs and tissues. The material obtained by puncture reveals a large number of pasmocytes.
The diagnosis is made based on 3 main criteria:
- Detection of plasma cells in the myelogram.
- Detection of monoclonal immunoglobulin in blood and urine tests.
- Organ damage associated with the development of the tumor process.
The main importance in diagnosis is the examination of a biopsy specimen and the detection of a tumor process in the organs and tissues of the human body. It allows you to identify patients with a symptomatic form of the oncological process.
Treatment

Today, treatment of multiple myeloma involves its control. A cure, at least a potential one, can only be discussed with a bone marrow transplant.
Plasmacytoma is a well-controlled disease; with early detection and proper treatment, long-term remission is possible. The initial stages of smoldering forms of the disease do not require immediate intervention. Conversely, the last stage requires rapid and intensive therapy to prolong the patient’s life.
Treatment of Rustitsky-Kahlen disease involves:
- Initial therapy.
- Supportive.
- Treatment of relapses and persistent forms.
The main method of treatment is chemotherapy (monochemotherapy, polychemotherapy). But this does not exclude the use of other methods:
- Stem cell transplantation (auto- and alletransplantation, that is, transplantation of one’s own or donor cells).
- Surgical intervention.
- Radiation therapy.
- Symptomatic measures.
Let's look at these treatment methods in more detail.
Operation
Surgery is performed when there is compression of internal organs or the spinal cord, which leads to severe disruption of the functioning of internal organs.
For spinal cord compression, lamyectomy (removal of the vertebral arch) and kyphoplasty in combination with treatment with Dexamethasone are practiced. In the case of a localized lesion (with solitary myeloma), surgery is also recommended, this time to remove the tumor.
Irradiation
The use of radiation therapy may be justified in cases of limited bone tissue lesions and high tumor resistance to chemotherapeutic agents. It is also recommended as palliative measures (maintaining quality of life) in patients who cannot take chemotherapy.
In what cases is radiation therapy prohibited:
- In severe renal failure.
- In older people.
- Physically weakened patients.
This method is often used to treat a pathological process localized in the facial bones of the skull.
Treatment of symptoms

Symptomatic therapy is designed to improve the patient’s quality of life and, if possible, eliminate the consequences of the tumor. It includes orthopedic care, medications: analgesics, hemostatics, drugs for correcting hypercalcemia. For acute anemia - erythropoietin or red blood cell transfusion.
Modern chemotherapy
It involves the use of several drug options for the treatment of generalized plasmacytomas. In some cases, one remedy is used, in others a combination of them is used.
The main medications are:
- Drugs for the treatment of multiple myeloma.
- Corticosteroids.
- Apoptosis inducers (drugs that trigger the self-destruction mechanism of tumor cells).
- Agents that stimulate immune cells and inhibit tumor cells.
Specific drugs for the treatment of plasmacytoma (Melphalan) are used as monotherapy or in combination with corticosteroids (Prednisolone). They are effective only in half of the cases.
Alkating cytostatics (Cyclophosphamide) give good results in combination therapy with the latest antitumor drugs and hormones. Their mechanism of action is based on the addition of a certain group to DNA, which is called alkyl. This prevents the altered cell from dividing and slows down the growth of the tumor.
Apoptosis inducers (Bortezomib) are used either alone or in combination with an antitumor agent and cortecosteroids. Its use does not eliminate the need for transplantation.
New cytostatics (Lenalidamide) combine antitumor properties with the ability to stimulate the body's immune cells. Their use in combination with hormones and alkalizing agents gives quite good results.
Treatment with Lenalidamide with other drugs extends the patient’s life by 4–5 years, while life expectancy with standard therapy averages from 1.5 to 3.5 years.
Thalidomide is considered a popular means of controlling generalized plasmacytomas. This drug is aimed at inhibiting pathological angiogenesis (the growth of blood vessels through the tumor, the formation of the oncological tissue’s own blood supply system). Good results are obtained by using Thalidomide with standard chemotherapy regimens.
Stages of treatment

The initial stage of therapy depends on the age of the patient and his condition. If the patient is under 65 years old and his general health allows, therapy is usually carried out in several steps:
- Preparation.
- High-dose chemotherapy.
- Transplantation of your own stem cells.
The first stage consists of induction therapy using new cytostatics (Bortezomib, Lenalidamide). Then high doses of Melphalan are administered and only then the transplantation is performed.
Not all patients can tolerate such treatment. Elderly, physically weakened or people with severe somatic illnesses are not able to withstand high doses of chemicals. They are prescribed low-dose combination therapy (Melfan + Prednisolone).
Maintenance therapy is designed to prolong the life of patients who have received high-dose therapy and undergone transplantation. Usually, new cytostatics are used for this, the same as those used at the preparatory stage of treatment.
Relapses of the disease occur in any case. Their treatment can be a repetition of the first course completed, including the use of transplantation. Or medications are prescribed that were not used in first-line therapy, that is, medications that have a different mechanism of influence on the cancer cell. Or the use of stronger agents that are aggressive to resistant pathological cells (Pomalidomide) is practiced.
As a rule, for therapy-resistant forms of Rustitsky-Kahlen disease, combined chemotherapy methods are used: cytostatics with Dexamethasone.
Forecast
If myeloma is in the first stage or smoldering or monoclonal gammopathy is diagnosed, patients live a long time (20–30 years) even without intensive courses of treatment. When diagnosed in the last stage of symptomatic myeloma, patients, even with treatment, live about 3–3.5 years. Recent innovations in pharmacology can extend this period to 5 years.
Unfortunately, to date, multiple myeloma has no effective treatment. So only timely diagnosis of the disease will allow a person to enjoy life longer.
Main symptoms of spinal cancer and diagnostic methods
Like any malignant tumor, spinal cancer is characterized by rapid growth of atypical cells. As a result, the symptoms of spinal cancer progress rapidly. The patient experiences not only pain, but also severe motor and neurological disorders.
The essence of pathology
As a matter of fact, from a medical point of view, in relation to the spine, the term “cancer” is not entirely appropriate. The fact is that cancer formation occurs from epithelial tissue cells, i.e. from the skin and mucous membranes. The spinal column is connective tissue - bones, cartilage, ligaments. Here there is a slightly different histological type of tumor - sarcoma. It can develop from both bones (osteosarcoma) and cartilage (chondrosarcoma).
In addition, in the lumen of the spinal canal formed by the vertebrae there is the spinal cord and its membranes. Various blastomas can form from the nervous tissue of the spinal cord - medulloblastomas, glioblastomas. Malignant spinal tumors can grow both from the substance of the spinal cord itself (intramedullary) and penetrate from the spinal membranes (extramedullary).
However, all these histological subtleties have almost no effect on the essence of the pathological process. Therefore, we will call all malignant tumors of the spine with the common term “cancer.” It should also be noted that sometimes the penetration of cancer into the spine is secondary, metastatic. This means that cancer cells are brought here by blood or lymph flow from other organs - stomach, lungs, liver, etc.

General manifestations
The insidiousness of spinal cancer is that the signs of this disease develop gradually, gradually. And the patient does not attach due importance to them until a certain time. He believes that he has osteochondrosis, lumbosacral radiculitis, and fatigue. As a result, precious time is lost, and in this case, delay is literally like death. The sooner you start treatment, the greater the chances of a favorable outcome.
Signs of spinal cancer include general and local manifestations, as well as neurological symptoms. General manifestations are weakness, decreased performance, often a moderate increase in temperature to subfebrile levels (370 - 380C). In later stages, the so-called cancer cachexia - exhaustion. The patient loses weight, muscle atrophy occurs, and the subcutaneous fat layer thins. Cachexia is accompanied by disruption of the functioning of all respiratory, circulatory, digestive, and internal secretion systems.
Local manifestations of spinal cancer are, first of all, pain. The pain is moderate at first, but in the final stages it becomes so unbearable that only drugs can eliminate it. In addition to pain, visible deformation of individual vertebrae and their spinous processes can be determined. Deformation of the vertebrae is sometimes accompanied by curvature of the entire spine - scoliosis. Often (but not always) a cancerous tumor can be determined by palpation (feeling) of the spine. Unlike benign tumors of the spine, cancer has an irregular shape, unclear contours, and is tightly fused to the surrounding tissues.
Neurological symptoms of cancer are caused by damage to the spinal cord, as well as the sensory and motor roots of the spinal nerves. These symptoms are characterized by neurological disorders of varying degrees - paresis and paralysis. Paresis (not to be confused with an incised wound or cut) is a partial, incomplete impairment of sensitivity and movement in a certain limb or area of the body. Characterized by limited range of motion, a feeling of numbness, and crawling. Paralysis or plegia is a complete lack of movement and sensitivity in the affected area. Simply put, paresis and plegia are different stages of the same process, in this case cancer.
Symptoms at different locations
Cervical region
The higher the malignant tumor of the spine is located, the wider the area of neurological disorders and the more pronounced the symptoms of cancer. In this regard, cancer of the cervical spine is most severe. Here, neurological disorders develop in all areas of the body located below the cervical tumor. First of all, this is paresis or plegia in all four limbs - the so-called. tetraparesis (tetraplegia). In the final stages of neck cancer, the thoracic intercostal muscles are paralyzed. As a result, it becomes difficult for the patient to breathe, and he is transferred to artificial ventilation (ALV), when breathing is carried out using a machine.
Due to compression of the spinal cord by the tumor, the circulation of the cerebrospinal fluid (CSF) is disrupted. As a result, cerebrospinal fluid accumulates in the ventricles of the brain, and intracranial pressure increases. This is accompanied by a severe headache, nausea, vomiting, impaired swallowing, varying degrees of loss of consciousness, even coma. For the cervical localization of the tumor, the so-called a symptom of a cerebrospinal fluid push - when pressing on the jugular veins of the neck, pain occurs at the location of the cancer. Another nonspecific sign of a violation of the outflow of cerebrospinal fluid is the occurrence of a headache when tilting the head forward.
Thoracic region
With thoracic cancer, paresis of the upper limbs, respiratory disorders, and disturbances in the functioning of the chest organs may develop. Here, too, much depends on the level of the tumor. Due to damage to the spinal cord and spinal nerve roots, the innervation of the heart, lungs, and diaphragm is disrupted. This is accompanied by palpitations, irregular heart rhythm, shortness of breath, and various digestive disorders. The back muscles in the area of the cancerous tumor are reflexively tense. Often such patients also need to be transferred to mechanical ventilation.
Lumbar region
With lumbar cancer, the pelvic organs, lower back and lower limbs are affected. Classic for this location of cancer is the so-called. cauda equina syndrome. The fact is that the spinal cord is shorter than the spinal canal - it ends somewhere at the level of the first lumbar vertebra. Below this level, the nerves passing through the spinal canal have the appearance of a bundle, resembling a horse's tail.
Sometimes the tumor can affect the fibers of the cauda equina. This is accompanied by symptoms such as:
- Intense burning pain in the lower back, radiating to the lower extremities
- Decreased muscle tone, paresis or plegia in both lower extremities
- Urinary incontinence
- Spontaneous defecation.
In addition, lumbar tumor leads to dysfunction of the genital organs. In men, this is manifested by difficulty in erection and ejaculation, in women – by various types of menstrual irregularities.
Diagnostic tests
Diagnosis of spinal cancer, like any disease, begins with an examination and interview of the patient. Already at this stage, the characteristic appearance (cachexia), complaints (pain in the spine) and neurological symptoms may lead the doctor to think about the presence of spinal cancer. But the clinical picture is not always so bright. As already mentioned regarding cancer, this disease is not only dangerous, but also insidious.
Therefore, special research methods are needed. Traditional radiography in 3 projections (direct, oblique and lateral) does not always allow recognizing a malignant process. Much more informative is layer-by-layer radiography performed on a computed tomograph (CT). However, even CT scans cannot always detect small tumors located deep within the spinal cord. In such cases, the most effective diagnostic method is nuclear magnetic resonance.
To clarify the nature of the tumor, a puncture (puncture) of the spinal canal is performed and cerebrospinal fluid is taken for laboratory tests. However, spinal puncture is possible only in the lumbar region, and in the overlying sections this intervention is associated with technical difficulties and a risk to the patient’s health. The prognosis for spinal cancer is always serious - the percentage of cases of disability and death is too high. It is believed that the outcome of cancer is favorable in cases where the patient, after timely and comprehensive treatment (chemotherapy, radiation therapy, surgery), lives for 5 years or more.
Comments
Sasha - 11.26.2014 - 14:25
- answer
Hera — 12/14/2014 — 22:11
- answer
Galina 65 years old - 09.30.2016 - 14:58
- answer
Guest — 03/06/2017 — 00:08
- answer
Add a comment
My spina.ru © 2012-2018. Copying of materials is possible only with a link to this site.
ATTENTION! All information on this site is for reference or popular information only. Diagnosis and prescription of medications require knowledge of the medical history and examination by a physician. Therefore, we strongly recommend that you consult a doctor regarding treatment and diagnosis, and not self-medicate. User AgreementAdvertisers
Tenosynovitis of the tendon: long head of the biceps, popliteus and biceps brachii
Orthopedists and traumatologists often encounter a specific lesion, which is defined as tendon tenosynovitis. The pathology is characterized by a long latent course, which reduces the likelihood of timely consultation with a doctor. The disease causes excessive tendon stiffness, swelling, and pain. Treatment is complicated if the presence of microcrystals of salts in the tendons is confirmed, and they themselves have undergone fiber disintegration.
Causes
The active development of the disease is facilitated by infection of adjacent tissues or the penetration of pathogenic microflora into the tendon structure. In 80% of cases this occurs due to a puncture or other violation of the integrity of the tendons. Main routes of damage:
- Existing infections, especially STIs (in 90% of cases of identified infectious tenosynovitis, the patient suffered from gonorrhea).
- Physical trauma, after which the acquired acute infection is divided into monomicrobial and polymicrobial. Each of them progresses depending on the nature and extent of the damage.
- Physiological aging process (common cause of patellar tenosynovitis).
- Staphylococcus aureus migrating from the epidermis, with which the patient was previously infected.
- Animal bite and subsequent suppuration of the bite wound.
- Intravenous use of hard drugs (tenosynovitis of the long head of the biceps tendon is likely to occur).
- Open damage to the skin, the surface of which was exposed to fresh or salt water with the presence of mycobacteria.

Any of the above methods leads to tenosynovitis. This includes situations where the patient has not completed the full course of treatment for rheumatoid or reactive arthritis.
Symptoms
An examination is enough for a doctor to make a preliminary diagnosis. And using diagnostic methods, the doctor confirms it, determining the nuances of the pathology.

Tenosynovitis of the tendon of the long head of the biceps brachii muscle is a stenotic disease that manifests itself as a specific pulling pain. In 9 out of 10 cases, the patient complains that an unpleasant sensation covers the shoulder and spreads along the front surface of the arm (along the biceps muscle). Palpation of the affected area gives a painful sensation: its localization is the groove between the tubercles of the humerus and in the direction below, where the tendon is even better accessible to palpation. Due to the pain, the patient has difficulty abducting his arm.

Tenosynovitis of the popliteus tendon is manifested by the following distinctive features:
- increase in pain after minor physical activity;
- extensive swelling around the knee joint;
- a clear hyperemia of the skin is visible.
Symptoms may be supplemented depending on the period of limitation of the lesion.
Diagnostics
Diagnosis of tendon tenosynovitis is difficult only because of the premature prescription of antibacterial therapy, which 60% of doctors carry out even before the final diagnosis is made. Laboratory research regarding the pathology in question is of secondary importance.
Methods for identifying tendon pathology are as follows:
- Laboratory research. In the blood, an increase in the content of leukocytes and an increase in ESR are established as indicators of an active inflammatory process.
- X-ray examination. The main goal of the method is to confirm the presence of tenosynovitis and exclude the concomitant development of osteomyelitis, bursitis, and arthritis.
- Ultrasound research. The method is informative and has advantages over MRI: low price, technical simplicity. Ultrasound does not involve the use of magnetic field energy. The procedure is safer for health and does not affect devices implanted inside the body (heart rate drivers). Ultrasound helps to study in detail the structures of tendons and ligaments, making it possible to differentiate tenosynovitis, including through the use of color Doppler mapping (CDC).
- MRI. The method provides an image of the entire joint, including the capsule with the glenohumeral ligaments, the articular cartilage on the head of the humerus. The muscles and tendons surrounding the joint and the synovial bursae are also visualized.
MRI and ultrasound of the shoulder or knee joint are not interchangeable diagnostic methods. The implementation of each of them involves specific goals and objectives.
Treatment
Delay in going to the hospital does not promise a positive prognosis - the disease progresses to an even more aggravated stage. Then the patient loses the opportunity to even self-care, and there is no need to talk about the implementation of work activity. One of the options for wasting time is the desire to normalize health using unofficial methods. Traditional medicine does not contain a single recipe that can restore the tendon-ligament apparatus. And patients taking decoctions and applying compresses to the body waste time, increasing the risk of developing disability.
Conservative
If the diagnostic results confirm that the existing disorder is tenosynovitis of the long head of the biceps tendon, treatment with conservative methods involves the following:
| Type of treatment, prescribed group of drugs | Purpose and features | Possible side effects |
| Non-steroidal anti-inflammatory drugs. Diclofenac, Nimesulide (Nise), Ibuprofen |
They reduce the spectrum of the inflammatory process and minimize pain. The listed medications are administered once a day for 10 days. | Gastropathy |
| Painkillers. Ketanov, Ketarol, Dexalgin, Analgin |
Analgesics are administered when NSAIDs are insufficiently effective, when pain in the limb persists. The drugs eliminate attacks of pain for 4-5 hours, which allows you to normalize your well-being and helps you cope with post-operative recovery. | Gastropathy, sleep disturbance, arrhythmia |
| Diuretics Furosemide, Lasix |
Therapy, the purpose of which is to reduce swelling. The dosage depends on the patient’s weight, the severity of edema | Lower back pain at the level of the kidneys |
| Antibiotic therapy Ceftriaxone, Ceftazidime |
Broad-spectrum antibiotics are prescribed if there is a proven relationship between tenosynovitis and an existing infection. The goal is to eliminate pathogenic microflora | Intestinal disorder |

To implement hormonal treatment, drugs from the glucocorticoid group are used - Dexamethasone and Prednisolone.
Injection of hormonal drugs, especially in chronic processes, does not provide a complete cure, increases the rate of collagen degradation, and negatively affects the production of new collagen (reduces its synthesis by 3 times).
The doctor expands general prescriptions with the active use of immunomodulatory agents and vitamin therapy.
More details

During conservative therapy, it is important not to load the affected joint; for this purpose, immobilization is performed with an orthosis. Local application of ointments is recommended: Nise, Dolobene, Ketonal.
Physiotherapy
Physiotherapeutic methods help normalize blood circulation, relieve or minimize pain, and improve metabolic processes in the affected area. Procedures that are advisable to prescribe if tenosynovitis of the biceps brachii tendon, popliteal fossa or other part is confirmed include magnetic therapy; laser therapy; applying thermal applications. The use of electrophoresis with novocaine will improve limb abduction and reduce pain.
Recently, radon baths have been actively used.
After the documented recognition of the safety of radon in the treatment of joint pathologies, interest in this gas is growing. The element’s demand is explained by its unique therapeutic capabilities.
Radon is an inert gas that is colorless and odorless. It is 7.5 times heavier than air, has 3 isotopes, the most important of which is 222 Yal with a half-life of 3.82 days.
Before performing radon baths, the doctor makes sure that the patient has no contraindications to the medical technology:
Among them:
- Fever of unknown origin.
- Oncological processes (confirmed) – the presence of malignant neoplasms, benign tumors that have a tendency to grow.
- All blood diseases.
- Heart rhythm disturbances (atrial fibrillation, extrasystole).
- Psycho-emotional disorders (epilepsy, neuroses, schizophrenia).
- Previous large-focal or multiple small-focal cerebral infarction.
- Professional activities associated with prolonged exposure to radioactive or electromagnetic radiation.
- The period of pregnancy and breastfeeding.
- Violation of the functional activity of the thyroid gland, high predisposition to its hyperfunction.
- Condition on the eve of surgery.
- Severe gynecological conditions - fibrocystic mastopathy, uterine fibroids, fibroids, adenomyosis, endometriosis.
- In men - prostate adenoma.
- Cholelithiasis.
- The presence of stones in any segment of the urinary system.
- Confirmed retinal detachment.
- The presence of defects on the skin, areas of weeping dermatitis, pathologies of fungal origin.
- Confirmed osteoporosis.
To determine the radon concentration for the procedure, the doctor is guided by the dominant pain manifestations. Dry air baths and traditional water baths are performed. The effect of the procedure is improved blood supply to the tissues adjacent to the joint; high probability of long-term pain relief (in 90% of cases).
Anton Epifanov about physiotherapy:
Surgery
Surgical intervention is performed in extreme cases when it is not possible to restore the limb using conservative methods. Surgical treatment is aggravated by the patient's age over 45 years, the presence of insulin-dependent diabetes mellitus, and if the etiology of tenosynovitis is the progression of a polymicrobial infection.
Tendon plastic surgery is a multi-stage, delicate operation. It involves subsequent long-term recovery and has a high price.
Treatment of joints Read more >>

The introduction of antibiotics a day before surgery and active intraoperative antibiotic therapy help eliminate the risk of complications in the postoperative period.
Features of anesthesia during surgery for tendon tenosynovitis:
- in the choice of anesthesia, the short duration of the intervention, the absence of the need for deep relaxation, and the presence of adequate hemostatic measures are important;
- modern medications provide adequate pain relief without threatening the patient’s life;
- A common complication after surgery is short-term post-anesthesia depression. It provides the possibility of early transfer of the patient from the ICU (intensive care ward) with patient activation;
- The depth of immersion in anesthesia is ensured by narcotic analgesics. In clinics with high financial support, they practice the most successful combination for anesthesia during short operations - Diprivan + narcotic analgesics (in 68% of cases). But the high cost of Diprivan limits its use in clinical practice. Hospitals with less funding use Ketamine for anesthesia. Its difference from Diprivan is specific: as patients recover from anesthesia, they need sedative therapy (carried out in standard dosages). It is important for the specialist to monitor the main vital signs - they must be stable throughout the entire surgical intervention.
- In 23.3% of cases, barbiturates were used for anesthesia, mainly sodium thiopental in standard dosages. If the depth of anesthesia was sufficient, “controllability” of anesthesia causes certain difficulties. Long-term post-anesthesia depression is possible, requiring constant monitoring of the patient.
The prognosis for recovery is favorable (subject to early seeking of medical help). However, the patient should prepare: full recovery will take 3-4 months.
Conclusion
Tenosynovitis of the tendon can only be cured in a hospital setting, and therefore by the methods of official medicine. It is not safe to rely on alternative options. The most common cause of pathology is chronic damage. Orthopedists and traumatologists are involved in eliminating the disease. If tenosynovitis is of infectious origin, a venereologist is involved in drawing up a treatment plan.